 Powered by Bioz
Powered by Bioz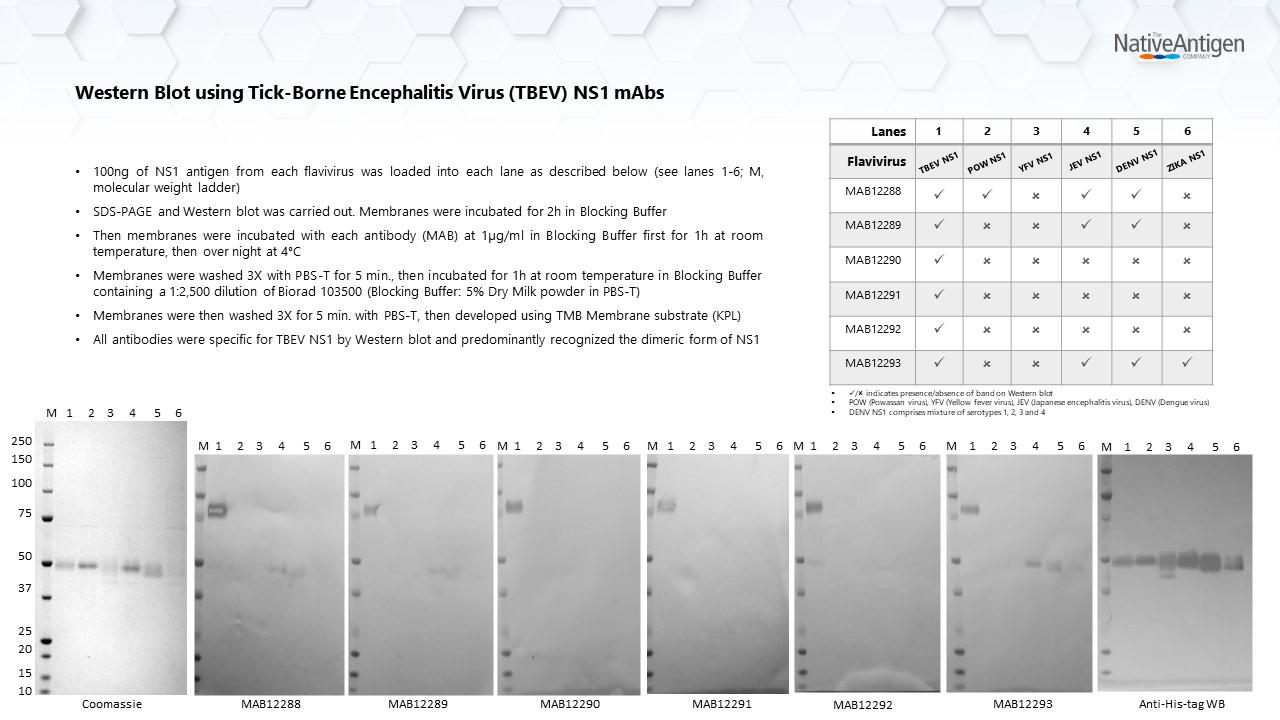

Price range: £292.93 through £735.04 excl. VAT
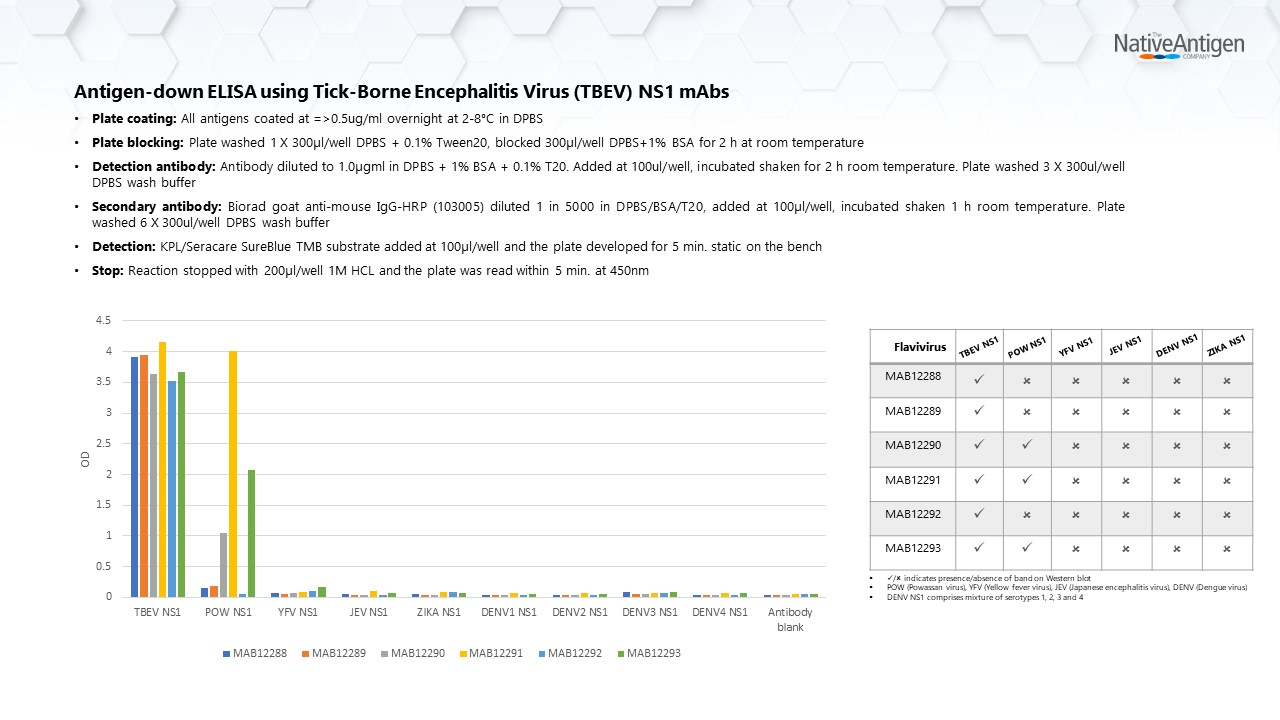
Mouse monoclonal antibody specific for Tick-borne Encephalitis Virus (TBEV) NS1 protein. This antibody recognises TBEV NS1 in Western blotting and ELISA assays. The antibody cross reacts with Powassan Virus NS1 in ELISA but not with other Flavivirus NS1 proteins tested.
Tick-borne Encephalitis Virus NS1 antibody (clone M837), is a mouse monoclonal antibody that recognises NS1 protein from Tick-borne Encephalitis virus (TBEV). This antibody predominantly recognises dimeric TBEV NS1 in Western blotting. In ELISA assays, the antibody cross reacts with Powassan Virus NS1 but does not cross react with other Flavivirus NS1 proteins tested.
Tick-borne encephalitis virus (TBEV) belongs to the genus Flavivirus, of the family Flaviviridae. The virus is primarily transmitted through the bite of infected hard ticks, of the family Ixodidae. Small rodents are the primary hosts for TBEV with humans acting as accidental hosts. The virus can also be transmitted to humans through unpasteurized milk in areas where TBEV is prevalent (CDC)
TBEV is a neurotrophic virus that causes tick-born encephalitis (TBE) in humans, affecting the central nervous system (CNS). TBE is endemic in many parts of Europe, China, Mongolia and the Russian Federation and is the most common tick-born CNS infection in these. Three subtypes of TBEV have been recognised that cause tick-borne encephalitis, which are European, Far-Eastern and Siberian.
TBEV infection is asymptomatic in most cases with some individuals presenting with influenza-like symptoms. In symptomatic cases, TBEV infection typically presents as meningitis, encephalitis or meningoencephalitis. A high percentage of acute TBE cases may also develop post-encephalitic syndrome with long-lasting neuropsychiatric symptoms or neurological dysfunction (Bogovic, P).
Diagnosis of TBE infection is primarily based on clinical presentation and serological testing for TBEV specific IgM and IgG antibodies in the patient’s serum and cerebrospinal fluid. There is no anti-viral treatment for TBEV. However, several effective vaccines for TBEV are currently available which are based on European and Far-Eastern strains of the virus (WHO)